Building an MLOps Infrastructure for 24/7 Clinical AI at a Hospital
The Problem
Quinze-Vingts Hospital generates thousands of ophthalmic exams every year across multiple devices — corneal topographers (MS-39), biomechanical analyzers (Corvis-ST), and clinical records entered by physicians. Each device produces data in its own format, its own coordinate system, its own units. None of them talk to each other. The data lives in CSV exports, proprietary databases, and handwritten notes.
Meanwhile, we’ve published research showing that ML models can predict surgical outcomes, classify corneal diseases, and identify high-risk patients with high accuracy. The gap between “this model works on a research dataset” and “clinicians can use this at 3 AM when they need it” is entirely an engineering problem. That’s what this infrastructure solves.
Architecture Overview
The system follows a medallion architecture — bronze, silver, gold, and serving layers — pulling from the hospital’s biomedical data lake where raw machine data is stored.
Bronze Layer: Data Integration
The hospital maintains a biomedical data lake containing raw exports from clinical devices. The bronze layer pulls data from this lake and integrates it with reconstructed data sources:
- MS-39 topography/tomography exports in their native formats
- Corvis-ST biomechanics raw device outputs
- Clinical records from physician databases
At this stage, data retains its original structure — the goal is reliable ingestion and basic validation, not transformation.
Silver Layer: Mathematical Transforms
The silver layer applies mathematical transformations that convert raw device data into computationally useful representations:
- Cartesian reconstruction: Converting polar-coordinate topographic grids into Cartesian spatial maps
- Zernike reconstruction: Decomposing elevation residuals into Zernike polynomial coefficients up to order 6, producing compact features that map to specific optical aberrations (I wrote about this in detail in my post on Zernike polynomials)
- Vector spaces: Transforming measurements into normalized feature vectors suitable for ML models
- Mathematical transformations: Other mathematical transformations specific to the domain (e.g., bidimensional astigmatism…) This is where the bulk of the domain-specific engineering happens — the transforms that turn device-specific outputs into ML-ready representations.
Gold Layer: Aggregated Datasets
The gold layer produces aggregate data tables and datasets ready for model training and analysis:
- 4,000+ features per patient computed across all data sources
- Validated, normalized, and joined on patient/exam identifiers
- Structured for both retrospective research (batch queries) and prospective inference (individual lookups)
- Quality-controlled with outlier detection and physiological bound validation
Serving Layer: Inference Applications
The serving layer hosts inference applications where ML models provide predictions to help clinicians in their diagnosis:
- TabPFN for multi-class diagnostic classification (88.7% accuracy across 7 corneal conditions in our recent BJO paper)
- CatBoost / XGBoost for surgical outcome forecasting and risk stratification
- ResNet / ViT for image-based topographic map analysis
We are currently testing these applications in Phase I of the validation phase, with clinicians evaluating model predictions against their diagnostic workflows.
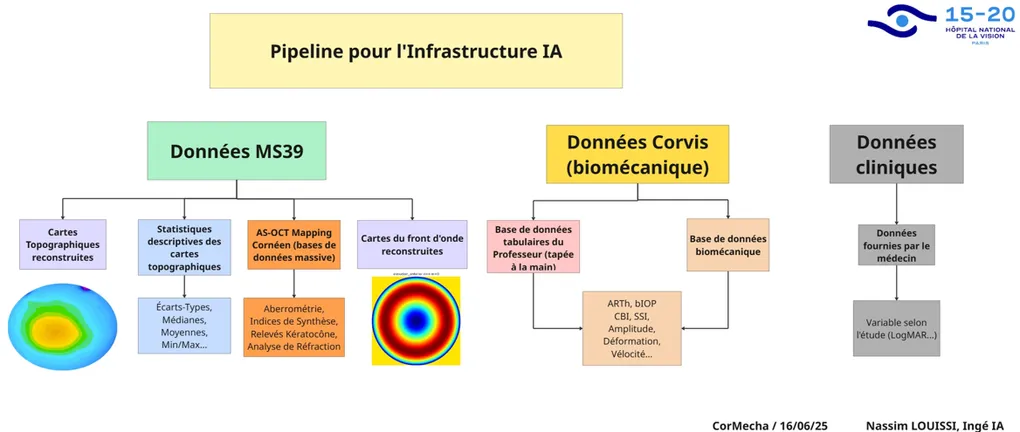
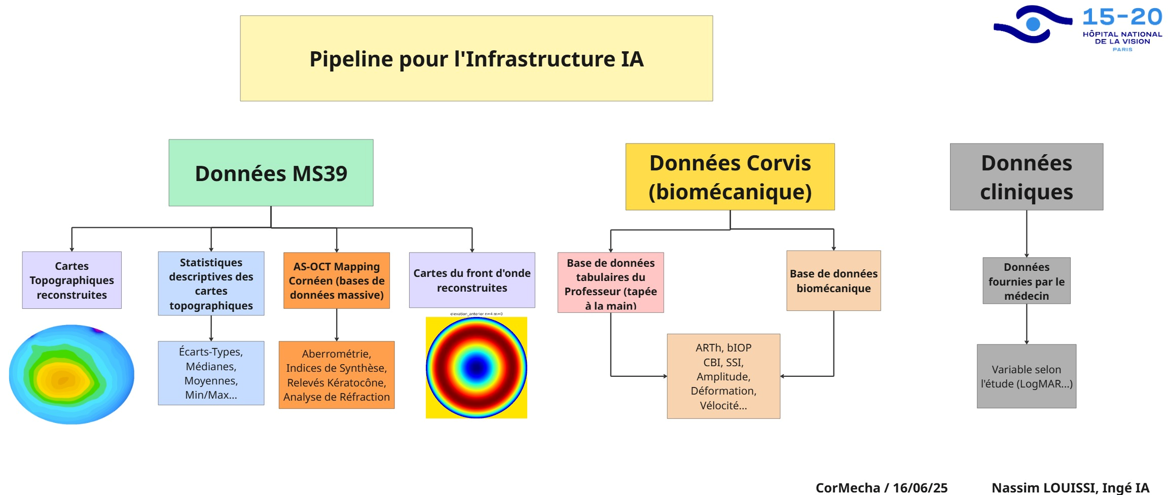
Data Sources
The pipeline integrates three heterogeneous data streams: corneal topography (MS-39), biomechanical analysis (Corvis-ST), and clinical records. Each comes with its own format, coordinate system, and validation challenges — polar-coordinate exports, proprietary device indices, and partially hand-entered physician records.
The engineering work involves coordinate conversions (polar to Cartesian), map reconstruction and validation against device outputs, statistical feature extraction (196 features per eye), symmetry computations between fellow eyes, unit standardization (Snellen to LogMAR), and outlier detection at multiple pipeline stages. Samples that fail validation are flagged for manual review rather than silently dropped.
Deployment
The serving layer runs on Docker containers, orchestrated with Kubernetes. Each model is packaged with its preprocessing pipeline — the same code that processes research data processes production data, so there’s no train/serve skew. The system is designed for 24/7 availability: a clinician can submit an exam and get a prediction at any hour, without an ML engineer in the loop.
Monitoring covers both infrastructure health (container status, latency, throughput) and model health (prediction distribution drift, feature value ranges, error rates). When the data distribution shifts — a new device firmware update, a change in acquisition protocol — the monitoring catches it before the predictions degrade.
The tricky part is that I had to build everything from scratch, which certainly creates technical debt for other engineers that are using the infrastructure. I’m currently working on the documentation of my work.
Challenges
Most ML in clinical research stops at the paper. A model gets trained on a curated dataset, performance metrics are reported, and the code goes into a repository that nobody touches again. The gap between that and a system a doctor can actually use is enormous:
- Data doesn’t arrive clean and can drift over time (Flynn effect)
- Devices get updated and export formats change
- Clinicians need trust and an understanding of the why
- It has to work at 3 AM
The infrastructure I’m building at Quinze-Vingts handles all of this.
What’s Next
The current system handles MS-39 and Corvis-ST data. The next phase is to include several other machines in order to increase the scope of the system.
Overall, this is my first End to End Machine Learning Production Infrastructure ever. It’s safe to say that it’s not easy. I’m glad I grinded through it. I’m thankful for the opportunity and I still have a lot to learn.
If you’re building similar systems — ML infrastructure or Production Pipelines — I’d like to hear about it. Connect on LinkedIn.